
Timisoara_Med 2022, 2022(1), 5; doi:10.35995/tmj20220105
Case Report
Single-Stage Decompression for Triple Nerve Entrapment of the Distal Upper Limb
1
Hardmed Medical Center, Plastic, Aesthetic and Reconstructive Microsurgery Office, 420127 Bistrița, Romania
2
Plastic Surgery and Reconstructive Microsurgery Department, Clinical Rehabilitation Hospital, 400347 Cluj-Napoca, Romania; oanacalinmorar@gmail.com (C.L.M.); mirolumi@gmail.com (L.M.)
*
Correspondence: bogdanioncioaia@gmail.com; Tel.: +40-743212961
How to cite: Ioncioaia, B.; Morar, C.L.; Miron, L. Single-stage decompression for triple nerve entrapment of the distal upper limb. Timisoara Med. 2022, 2022(1), 5; doi:10.35995/tmj20220105.
Received: 16 March 2022 / Accepted: 27 April 2022 / Published: 15 June 2022
Abstract
:Peripheral nerve injuries have a significant negative impact on daily activities and quality of life. Considering that the compression of more than one peripheral nerve may have an increased negative emotional impact, it is, therefore, important to make a thorough diagnosis and speed up the surgical treatment. We present the case of a 71-year-old male patient with multiple simultaneous compression neuropathies of the distal right arm involving the posterior interosseous, median and ulnar nerves, who sought medical care during the first year of the COVID-19 outbreak.
Keywords:
peripheral nerve entrapment; upper extremity; posterior interosseous nerve; median nerve; ulnar nerve; hand surgeryIntroduction
Peripheral nerve injuries have a significant negative impact on daily activities and quality of life [1]. Carpal tunnel syndrome (CTS) represents the most frequent entrapment of peripheral nerves, followed by cubital tunnel syndrome (CS) [2,3,4,5]. The compression of the posterior interosseous nerve (PIN) is specific to the dorsal proximal region of the forearm, with a higher incidence in women and a more common involvement of the right upper extremity [6]. Considering that the compression of more than one peripheral nerve may have an increased negative emotional impact, it is, therefore, important to speed up both diagnosis and surgical treatment [1]. However, in such instances, it is not clear whether a serial or a all-in-one approach would be more beneficial for patients.
Case Report
A 71-year-old, right-handed, male patient presented to our outpatient clinic with proximal forearm pain, paresthesia and mild extension deficit of the 2nd through the 5th finger of his right hand. The onset of symptoms began three months earlier after a fall on his right upper extremity.
The clinical examination of his right upper extremity revealed thenar and hypothenar atrophy, mild extension deficit of all five fingers, adduction deficit of the thumb, hypoesthesia in the ulnar nerve territory, resting and triggered pain at palpation and percussion in the proximal one third of the dorsal forearm and posterior to the medial epicondyle.
Ultrasound revealed morphological changes to the posterior branch of the radial nerve at the level of the supinator arcade (PIN). A cervical MRI showed multiple degenerative lesions of the dorsal vertebral disc and foraminal compression of the left C5-C6 and C7-C8 nerve roots. Nerve conduction studies (NCS) objectified a lesion of the PIN and ulnar nerve at the medial elbow but no deficit of the median nerve at the level of the wrist.
The surgical treatment of the patient was postponed due to the national state of emergency issued by the Romanian Government due to the COVID-19 pandemic outbreak, and he was readmitted for surgical treatment four months later after a drop in COVID-19 incidence. In the meantime, the patient developed an additional adduction deficit of the 5th finger, opposition deficit of the 5th finger, decreased active flexion and extension at the radiocarpal joint against a resistance elicited by the examiner and pain at percussion of the medial epicondyle with distal irradiation.
Additionally, a subcutaneous, painless, tumoral mass with a 2 cm diameter, which was not previously observed, was noted in the volar distal third of the forearm. The patient noticed its growth in the 4 months preceding his readmission. A positive Durkan and Phalen test was obtained. An ultrasound examination described a well-defined, hypoechogenic mass beneath the transverse carpal ligament (2.5 cm length and 1.5 cm width), without hypervascularization but with the partial compression of the median nerve in the carpal tunnel.
Triple compressive neuropathy of the PIN (at the arcade of Frohse), ulnar nerve (cubital tunnel syndrome) and median nerve (CTS) of the distal upper extremity was diagnosed.
The surgical intervention was performed in an axillary block, with arm tourniquet.
The PIN was approached via a posterior antebrachial incision, using the brachioradialis (BR) and extensor carpi radialis longus (ECRL) interval. Compression of the PIN was observed at the entrance point into the arcade of Frohse, with a neuroma proximal to it (Figure 1). Surgical decompression of the PIN was undertaken, followed by the digital exploration of the radial nerve proximally to a point above the lateral epicondyle.
Next, the decompression of the ulnar nerve at the level of the medial elbow was performed. The ulnar nerve was exposed through a 10 cm axial incision on the medial aspect of the elbow, first proximal to the cubital tunnel and continued distally to the flexor carpi ulnaris (FCU) arcade. (Figure 2). The ulnar nerve was anteriorly transposed and wrapped in an adipofascial flap for mechanical protection.
Lastly, the volar wrist mass was approached via a volar incision at the distal third of the forearm (Figure 3). The tumor extended into the carpal tunnel, adhered to the epineurium of the median nerve but was uneventfully excised and sent for histopathological examination. The median nerve presented mild local changes due to the compression by the tumor. External neurolysis and epineurotomy were performed, followed by coverage of the median nerve with a hypothenar adipose flap. Prior to wound closure, lavage and hemostasis were achieved with a maximum tourniquet time of 90 min.
No additional motor or significant sensory deficits occurred postoperatively. The patient was encouraged to pursue hand rehabilitation after hospital discharge. The histopathological exam reported a lipoma.
Postoperative follow-up and hand therapy were cumbersome due to the COVID-19 pandemic and its subsequent national restrictions. At 8 months follow-up, the patient presented with weakened pinch and grip, and the persistence of extension deficit accompanied by the inability to flex the DIP joints into the palm. Stiffness of the metacarpophalangeal and proximal interphalangeal joint of the 1st to 5th fingers was noticed. The sensory recovery for the ulnar nerve was identified as S2+ and S1 for the median nerve according to the modified Medical Research Council Scale for Sensory Recovery.
The NCS revealed normal function for the median and ulnar nerves, while for the PIN, the reinnervation had reached the extensor indicis muscle. The patient was referred to a hand therapist for intensive hand rehabilitation.
Discussion
Simultaneous peripheral nerve entrapment in the distal upper limb is usually associated with carpal tunnel and cubital tunnel syndromes [7]. To date, we are not aware of any reported cases of multiple concomitant compression neuropathies of individual nerves at this level in the literature.
While singular clinical manifestations of median, posterior interosseous or ulnar nerve entrapment may be somewhat evident, NCS are usually necessary to confirm the presence and degree of nerve injury in cases of multiple involvement [6,8]. Although the clinical manifestations of PIN and cubital nerve entrapment could be correlated with the NCS, median nerve compression syndrome was not noticed preoperatively in nerve conduction studies. Ultimately, ultrasound revealed a space occupying lesion adhering to the median nerve as the cause of the nerve compression, which was confirmed by the uneventful excision.
As an adjuvant procedure to the open carpal tunnel decompression, we generally use the hypothenar adipose flap for median nerve coverage, since many of our patients have advanced stages of median nerve compression [9]. Although the use of the hypothenar flap is recommended by some authors in cases of recurrence, we believe that it offers the advantage of mechanical protection to the already scarred median nerve during the movement of the radiocarpal joint, and contributes to its healing and the prevention of recurrence [10,11,12].
Although the current trend of surgical management of cubital tunnel consists of in situ decompression, we have not observed any recurrences in our cases when we have used the extended decompression approach with the subcutaneous transposition of the ulnar nerve, obtaining similar results to those reported by other authors [13,14].
In terms of surgical approach for the PIN, we preferred the dorsal approach using the BR-ECRL interval for the comfortable identification of the compression site at the arcade of Frohse [15,16].
Ultrasound and NCS remain helpful tools for the evaluation of the nerve morphology, physiology and etiology of nerve compression syndromes [17].
It is well known that regardless of the skillfulness of the surgeon, hand rehabilitation after peripheral nerve surgery is crucial, because the incompliance of the patient with their prescribed hand rehabilitation regimen may render the surgeon’s efforts useless.
Conclusion
Clinical examination coupled with NCS and ultrasound is important for a comprehensive diagnosis of upper limb nerve entrapment, especially when multiple nerves are involved. One-stage surgical decompression for the multiple nerve entrapment of the distal upper limb offers the benefit of a single hospital admission, reduced healthcare costs and a faster rehabilitation. Hand rehabilitation is essential and should follow all nerve surgery on the upper extremity.
Author Contributions
Conceptualization, B.I. and C.L.M.; Methodology, B.I. and C.L.M.; Software, B.I.; Validation, B.I., C.L.M. and L.M.; Formal Investigation, B.I. and C.L.M.; Resources, B.I. and L.M.; Data Curation, B.I. and L.M.; Writing—Original Draft Preparation, B.I. and C.L.M.; Writing—Review and Editing, B.I., C.L.M. and L.M.; Visualization, B.I. and L.M.; Supervision, C.L.M.; Project Administration, B.I.
Funding
This research received no external funding
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Wojtkiewicz, D.M.; Saunders, J.; Domeshek, L.; Novak, C.B.; Kaskutas, V.; Mackinnon, S.E. Social impact of peripheral nerve injuries. HAND 2015, 10, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Bickel, K.D. Carpal tunnel syndrome. J. Hand Surg. Am. 2010, 35, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Thatte, M.R.; Mansukhani, K.A. Compressive neuropathy in the upper limb. Indian J. Plast. Surg. 2011, 44, 283–297. [Google Scholar] [CrossRef] [PubMed]
- Kim, P.T.; Lee, H.J.; Kim, T.G.; Jeon, I.H. Current approaches for carpal tunnel syndrome. Clin. Orthop. Surg. 2014, 6, 253–257. [Google Scholar] [CrossRef] [PubMed]
- Palmer, B.A.; Hughes, T.B. Cubital tunnel syndrome. J. Hand Surg. Am. 2010, 35, 153–163. [Google Scholar] [CrossRef] [PubMed]
- Wheeler, R.; DeCastro, A. Posterior Interosseous Nerve Syndrome; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Shulman, B.; Bekisz, J.; Lopez, C.; Maliha, S.; Mahure, S.; Hacquebord, J. The association between concomitant ulnar nerve compression at the elbow and carpal tunnel syndrome. HAND 2020, 15, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Staples, J.R.; Calfee, R. Cubital tunnel syndrome: Current concepts. J. Am. Acad. Orthop. Surg. 2017, 25, e215–e224. [Google Scholar] [CrossRef] [PubMed]
- Strickland, J.W.; Idler, R.S.; Lourie, G.M.; Plancher, K.D. The hypothenar fat pad flap for management of recalcitrant carpal tunnel syndrome. J. Hand Surg. Am. 1996, 21, 840–848. [Google Scholar] [CrossRef]
- Kanchanathepsak, T.; Wairojanakul, W.; Phakdepiboon, T.; Suppaphol, S.; Watcharananan, I.; Tawonsawatruk, T. Hypothenar fat pad flap vs conventional open release in primary carpal tunnel syndrome: A randomized controlled trial. World J. Orthop. 2017, 8, 846–852. [Google Scholar] [CrossRef] [PubMed]
- Giunta, R.; Frank, U.; Lanz, U. The hypothenar fat-pad flap for reconstructive repair after scarring of the median nerve at the wrist joint. Annales de Chirurgie de la Main et du Membre Supérieur 1998, 17, 107–112. [Google Scholar] [CrossRef]
- Goitz, R.J.; Steichen, J.B. Microvascular omental transfer for the treatment of severe recurrent median neuritis of the wrist: A long-term follow-up. Plast. Reconstr. Surg. 2005, 115, 163–171. [Google Scholar] [PubMed]
- Yahya, A.; Malarkey, A.R.; Eschbaugh, R.L.; Bamberger, H.B. Trends in the surgical treatment for cubital tunnel syndrome: A survey of members of the American Society for Surgery of the Hand. HAND 2018, 13, 516–521. [Google Scholar] [CrossRef] [PubMed]
- Hutchinson, D.T.; Sullivan, R.; Sinclair, M.K. Long-term reoperation rate for cubital tunnel syndrome: Subcutaneous transposition versus in situ decompression. HAND 2019, 16, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Moradi, A.; Ebrahimzadeh, M.H.; Jupiter, J.B. Radial tunnel syndrome, diagnostic and treatment dilemma. Arch. Bone Jt. Surg. 2015, 3, 156–162. [Google Scholar] [PubMed]
- Kim, D.H.; Murovic, J.A.; Kim, Y.Y.; Kline, D.G. Surgical treatment and outcomes in 45 cases of posterior interosseous nerve entrapments and injuries. J. Neurosurg. 2006, 104, 766–777. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.V.; Wu, W.T.; Özçakar, L. Ultrasound imaging and guidance in peripheral nerve entrapment: Hydrodissection highlighted. Pain Manag. 2020, 10, 97–106. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The posterior interosseous nerve after releasing the arcade of Frohse. Neuroma in continuity can be observed before the PIN enters the arcade.
Figure 1.
The posterior interosseous nerve after releasing the arcade of Frohse. Neuroma in continuity can be observed before the PIN enters the arcade.

Figure 2.
The ulnar nerve after releasing Osborne’s ligament and flexor carpi ulnaris aponeurosis.
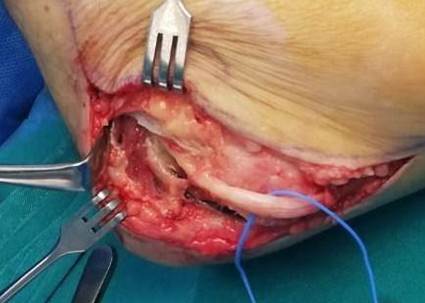
Figure 3.
The lipoma exiting the carpal tunnel.

© 2022, Copyright by the authors Licensed as an open access article using a CC BY 4.0 license