
Timisoara_Med 2022, 2022(2), 5; doi:10.35995/tmj20220205
Original Paper
The Comparative Analysis of Landsberg and Friedman and Stammberger and Hawke Computer Tomography Classifications in the Superior Attachment of the Nasal Uncinate Process (SAUP) and Potential Pitfalls in Evaluation
1
Faculty of Medicine, Muğla Sıtkı Koçman University, 48000 Muğla, Turkey
2
Training and Research Hospital, 48000 Muğla, Turkey; celibol1068@e-mail.com
*
Correspondence: emrahdogan@mu.edu.tr; Tel.: +90-5066619794
How to Cite: Doğan, E.; Elibol, C. The comparative analysis of Landsberg and Friedman and Stammberger and Hawke CT classifications in the superior attachment of the nasal uncinate process (SAUP) and potential pitfalls in evaluation. Timisoara Med. 2022, 2022(2), 5; doi:10.35995/tmj20220205.
Received: 10 February 2022 / Accepted: 3 June 2022 / Published: 30 September 2022
Open access
: TIMISOARA MEDICAL JOURNAL is a peer-reviewed open-access journal.Abstract
:(1) Object: Our study aims to identify the common and diverging points in the superior attachment of the nasal uncinate process (SAUP) classifications and to draw attention to the pitfalls in these evaluation processes. (2) Material and Methods: This study was performed on 200 patients (males/females, 100/100; mean age/range: 37.13 ± 16.14/16–84), and 400 sides were bilaterally evaluated. Potential pitfalls were investigated. All UPs were classified according to the Landsberg and Friedman (LF) and Stammberger and Hawke (SH) classifications, and these two classifications were compared. (3) Results: There was a high statistically significant correlation between SH and LF. SH Type IV and LF Type 0 and SH Type III and LF Type 6 completely overlapped. SH Type I corresponded to LF Types 2 and 3 and SH Type II to LF Type 2, 3, 4, and 5 groups. There was no significant difference between genders or sides (right and left) in terms of the LF or SH classifications. (4): Conclusions: Following the thick band and paying attention to concavity and convexity helps to accurately evaluate the anatomical structure. Only two groups overlapped one to one. For SH Types II and III, and LF Types 1, 2, 3, 4, and 5, knowing the SAUP group in one classification does not give an exact idea about the group of the other classification. Therefore, it is not possible to make comparisons between reports or studies using different classifications.
Keywords:
paranasal sinus; uncinate process; maxillofacial; computed tomographyIntroduction
The uncinate process (UP) has high anatomical diversity, including variations such as bullous variants, medial/lateral deviations, and the superior attachment of the uncinate process (SAUP). It is essential for surgeons to know the anatomical variations in this region before an operation, especially in functional endoscopic sinus surgery (FESS), to avoid complications. The primary method used in the radiological evaluation of the paranasal region is computed tomography (CT) [1,2].
The nasal uncinate process (NUP), together with the middle turbinate, is among the key parts that form the ostiomeatal complex (OMC). It is the first anatomical barrier surgeons encounter when entering the nasal cavity [3,4]. The NUP is usually removed during endoscopic sinus surgery (ESS). This technique is known as uncinectomy. In the presence of a post-operative remnant, the frontal FESS procedure terminates with failure. Therefore, SAUP has great importance in the management of ESS. It is necessary to know where the NUP attaches in order not to damage the ethmoid roof [5]. The easiest way in radiological reporting is to specify the SAUP as lamina papyracea, middle turbinate, or skull base. However, there are two different classifications formally for this subject, known as the Landsberg and Friedman (LF) and Stammberger and Hawke (SH) classifications [6,7]. SH types are denoted by roman and LF types by arabic numerals. The LF classification includes four groups, and SH comprises six groups [6,7]. Different classifications have been used in studies. For example, Barosso [8], Srivastava [7], and Doğan [9] used the LF classification, while Güngör [6], Kansu [5], and Ercan [10] used the SH classification in their studies. This situation creates confusion, makes comparison difficult, and prevents a healthy meta-analysis study. The last meta-analysis study in the English literature on this subject belongs to Papadopoulos in 2021 [1]. In this study, variations in almost all points of the paranasal region were compared. However, the NUP part was probably overlooked due to this situation [1].
To the best of our knowledge, in our study, SAUP classifications (LF and SH) are compared for the first time. In addition, having a confusing anatomical structure with ethmoid cells and many variations makes it difficult to follow the NUP, especially on the roof, thus causing non-standard subjective evaluations. In the Material and Methods section, the common pitfalls of SAUP evaluations are also emphasised. Our study aims to identify the common and diverging points in SAUP classifications and to draw attention to the pitfalls in these evaluation processes.
The uncinate process is a hook-shaped structure and is one of the four anatomical regions called by the same name in the body. Apart from the NUP, a part connected with the head of the pancreas is called the uncinate. In addition, there is a neural tract in the brain called the uncinate fasciculus. Furthermore, there is an uncinate process of the cervical vertebra. Therefore, the abbreviation used is the nasal uncinate process (NUP) instead of the uncinate process (UP), unlike other studies [11,12,13]. Our study aims to identify the common and diverging points in the superior attachment of the nasal uncinate process (SAUP) classifications and to draw attention to the pitfalls in these evaluation processes.
Material and Methods
This study was approved by the Muğla Sıtkı Koçman University Human Research Ethics Committee with the document number 200022/2020. Between January 2018 and December 2020, 239 healthy patients who underwent paranasal CT scans for various indications were retrospectively evaluated. All the images were obtained from picture-archiving communication systems (PACSs). Thirty-two patients were excluded from the study for the following medical reasons: six patients had a history of uncinectomy operation, two had polyposis, four had rhinitis, eleven had sinusitis, four had major deviation, one had NUP medialisation, two had NUP lateralisation, and two had ethmoid hypoplasia. In addition, seven CTs with artefacts were not appropriate for evaluation. They were also excluded from the study. In total, 200 patients were accepted for general evaluation, and 400 sides were bilaterally evaluated. Power analysis was performed with the G-power test. The sample group was calculated at 44 for 95% power, 0.05 alfa, and 0.2 beta parameters. In conclusion, our study population size was fairly sufficient for analysis.
CT scans were performed with a 256-slice multi-detector CT scanner (Somatom, Siemens Healthcare, Erlangen, Germany). The patients’ position was prone, with the head in extension; the slice thickness for coronal imaging was 1.5 mm, and for axial imaging, it was 1 mm. The slices were perpendicular to the intraorbital meatal line, with dose parameters of 100 KVp and 40 MAs. The evaluation was performed at a workstation with a high-resolution medical monitor in a paranasal window (window width (WW): 2000–2400 Hounsfield unit (HU), window level (WL): 400–450 HU) and bone window (WW: 1800 HU, WL: 400 HU). The palatine bone for coronal imaging and the orbitomeatal line for axial imaging were taken as the reference lines. The CT sections started from the anterior wall of the frontal sinuses and ended with the posterior wall of the sphenoidal sinus.
All the images were independently assessed by two experienced radiologists on the coronal, axial, and sagittal planes. In case of contradictory results, the images were evaluated by both radiologists together.
The data were stored in a Microsoft Office Excel file (Excel 2010, Microsoft). We used the SPSS software (version 22.0, IBM) for statistical analysis. Continuous variables are expressed as mean ± standard deviation (SD) values. Qualitative variables were counted and calculated as percentages. All data were statistically compared according to gender. The Pearson chi-square (χ2) analysis and the Spearman and Kendall tau b test were used to evaluate the relationship between the variables. P values < 0.05 were considered statistically significant, and values of <0.01 were highly significant.
Classifications
The parameters used in the classification were as follows:
SH classifications:
- Type I: NUP bends laterally in its uppermost portion to be inserted into the lamina papyracea;
- Type II: NUP superiorly extends to the roof of the ethmoid, which is the skull base;
- Type III: The superior end of NUP medially turns and is attached to the middle turbinate;
- Type IV: Free NUP [14].
LF classifications:
- Type 1: Insertion into the lamina papyracea;
- Type 2: Insertion into the posterior wall of the Agger nasi cell;
- Type 3: Insertion into the lamina papyracea and junction of the middle turbinate with the cribriform plate;
- Type 4: Insertion into the junction of middle turbinate with the cribriform plate;
- Type 5: Insertion into the skull base;
- Type 6: Insertion into the middle turbinate [15].
Modified LF classification:
Figure 1.
(A) In anterior sections, the lower wall of the agger nasi cell mimics NUP (pseudo NUP appearance). In this case, SAUP is mistakenly interpreted as (SH/LF) Type III/6. (B) However, in posterior sections, it is seen that the NUP attaches to the base of the skull on the right and the orbit via an ethmoid bulla on the left. The right should be considered as (SH/LF) Type II/5, the left as LF Type 2. The SH equivalent is Type I since it is indirectly linked with the orbit wall via ethmoid cell.
Figure 1.
(A) In anterior sections, the lower wall of the agger nasi cell mimics NUP (pseudo NUP appearance). In this case, SAUP is mistakenly interpreted as (SH/LF) Type III/6. (B) However, in posterior sections, it is seen that the NUP attaches to the base of the skull on the right and the orbit via an ethmoid bulla on the left. The right should be considered as (SH/LF) Type II/5, the left as LF Type 2. The SH equivalent is Type I since it is indirectly linked with the orbit wall via ethmoid cell.
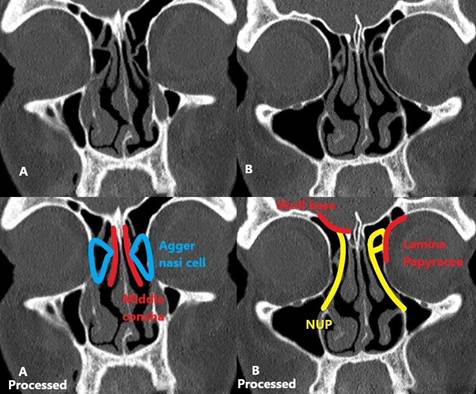
Figure 2.
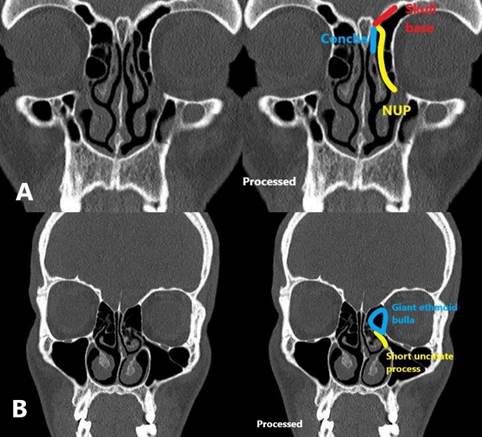
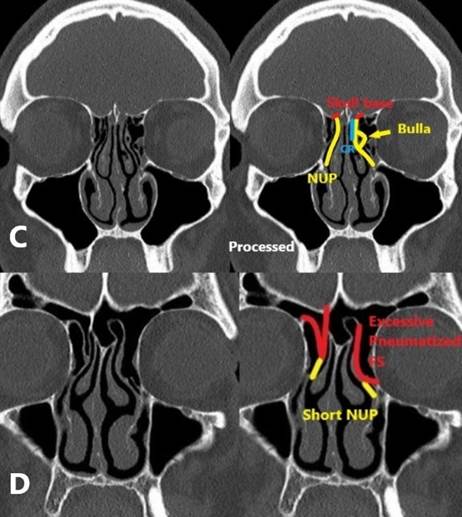
(A) NUP can attach to the border points of anatomical landmarks. This situation has an equivalent called Type 4 in the LF classification. According to SH, NUP is between Types II and III. Herein, the convexity direction should be considered. Since the direction is towards the base of the skull, SAUP should be considered SH Type II. (B) If the patient has a giant ethmoid cell, the NUP is usually short and merges with the ethmoid bulla. It is considered as (LF/SH) Type 2/I since NUP is connected with the orbital wall via ethmoid bulla. (C) Sometimes, the bullous variant-like cellular areas are seen on the course of the NUP. In this case, the cell insertion or bony part after the cell is taken into account. In the sample, the left side was considered Type II-5 because of insertion after cell. (D) In the case of excessive pneumatisation of frontal sinuses (FS), NUP is short. Attachment is in the base of FS. It should be considered (SH/LF) Type II/5. If the FS base is supposed to be a roof, the image can be evaluated as a separated NUP. LF Type 3 covers two-armed NUP attachments. The equivalent of this group is not present in SH. In these cases, the procedure needed is to follow the thick arm.
Figure 2.
(A) NUP can attach to the border points of anatomical landmarks. This situation has an equivalent called Type 4 in the LF classification. According to SH, NUP is between Types II and III. Herein, the convexity direction should be considered. Since the direction is towards the base of the skull, SAUP should be considered SH Type II. (B) If the patient has a giant ethmoid cell, the NUP is usually short and merges with the ethmoid bulla. It is considered as (LF/SH) Type 2/I since NUP is connected with the orbital wall via ethmoid bulla. (C) Sometimes, the bullous variant-like cellular areas are seen on the course of the NUP. In this case, the cell insertion or bony part after the cell is taken into account. In the sample, the left side was considered Type II-5 because of insertion after cell. (D) In the case of excessive pneumatisation of frontal sinuses (FS), NUP is short. Attachment is in the base of FS. It should be considered (SH/LF) Type II/5. If the FS base is supposed to be a roof, the image can be evaluated as a separated NUP. LF Type 3 covers two-armed NUP attachments. The equivalent of this group is not present in SH. In these cases, the procedure needed is to follow the thick arm.
Results
In total, 200 patients (males/females, 100/100; mean age/ range: 37.13 ± 16.14/16–84) were included in this study. In all the patients, 400 NUPs were evaluated according to SAUP classifications: 200 on the right side and 200 on the left side.
On the right side, according to the SH classification, 72/200 (36%) of the patients had Type I SAUP, 90 (45%) had Type II, 25 had Type III (12.5%), and 13 had Type IV (6.5%). In the evaluation of the same NUPs according to the LF classification, 13 (6.5%) of the patients had Type 0, 14 (7%) had Type 1, 63 (31.5%) had Type 2, 8 (4%) had Type 3, 34 (17%) had Type 4, 43 (21.5%) had Type 5, and 25 (12.5%) had Type 6 SAUP (Table 1).

Table 1.
The distribution of SAUPs according to SH and LF classifications on the right side.
| Type LF/SH | T 0 | T1 | T2 | T3 | T4 | T5 | T6 | Total |
|---|---|---|---|---|---|---|---|---|
| Type I | - | 14 | 58 | - | - | - | - | 72 |
| Type II | - | - | 5 | 8 | 34 | 43 | - | 90 |
| Type III | - | - | - | - | - | - | 25 | 25 |
| Type IV | 13 | - | - | - | - | - | - | 13 |
| Total | 13 | 14 | 63 | 8 | 34 | 43 | 25 | 200 |
The equivalents of all the LF Type 0 SAUPs were ST Type IV. All patients with LH Type 1 were in the SH Type I group. However, 58/63 of the patients with LF Type 2 were SH Type I, and 5/63 of them were SH Type II. LF T3, T4, and T5 were completely included in the SH Type II group. However, the majority of SH Type II group were in the LF T4 and T5 groups. Type II was the most inhomogeneous group. The patients were distributed among four separate groups, namely LF T2, 3, 4, and 5. All the LF T6s were Type III.
On the left side, 98 (49%) of the patients had Type I SAUP, 67 (33.5%) had Type II, 24 had Type III (12%), and 11 had Type IV (5.5%) according to the SH classification. In the LF classification, 11 (5.5%) of SAUPs were Type 0, 8 (6.5%) were Type 1, 93 (46.5%) were Type 2, 11 (5.5%) were Type 3, 20 (10%) were Type 4, 33 (16.5%) were Type 5, and 24 (12%) were Type 6 (Table 2).
Table 2.
The distribution of SAUPs according to SH and LF classifications on the left side.
| Type LF/SH | T 0 | T1 | T2 | T3 | T4 | T5 | T6 | Total |
|---|---|---|---|---|---|---|---|---|
| Type I | - | 8 | 90 | - | - | - | - | 98 |
| Type II | - | - | 3 | 11 | 20 | 33 | - | 67 |
| Type III | - | - | - | - | - | - | 24 | 24 |
| Type IV | 11 | - | - | - | - | - | - | 11 |
| Total | 11 | 8 | 93 | 11 | 20 | 33 | 24 |
In total, according to SH, 170/400 (42.5%) were Type I, 157/400 (39.25%) were Type II, 48/400 (12%) were Type III, and 24/400 (6%) were Type IV. According to LF, 24/400 (6%) were Type 0, 22/400 (5.5%) were Type 1, 156/400 (39%) were Type 2, 19/400 (4.75%) were Type 3, 54/400 (13.5%) were Type 4, 76/400 (19%) were Type 5, and 48/400 (12%) were Type 6.
In comparison, the following observations were made:
- SH Type I: 22/170 (12.9%) were Type 1, while 148/170 (87.1%) were Type 2 according to LF;
- SH Type II: 8/157 (5.1%) were Type 2, 19/157 (12.1%) were Type 3, 54/157 (34.4%) were Type 4, and 76/157 (48.4%) were Type 5 according to LF;
- SH Type III and Type IV: all the patients were, respectively, in Type 6 and Type 0 groups according to LF (Table 3).
Table 3.
The comparison of classifications.
| Stammberger type (n:400) | Landsberg and Friedman (n:400) | Overlap ratio (%) | ||
|---|---|---|---|---|
| Type | Number | Type | Number | |
| Type I | 170 | Type 1 | 22 | |
| Type 2 | 148 | I/2 = 87.05% | ||
| Type II | 157 | Type 2 | 8 | |
| Type 3 | 19 | II/5 = 48.4% | ||
| Type 4 | 54 | |||
| Type 5 | 76 | |||
| Type III | 48 | Type 6 | 48 | III/6 = 100% |
| Type IV | 24 | Type 0 | 24 | IV/0 = 100% |
SH and LF classifications were separately compared using the Pearson chi-square (χ²) and the Spearman and Kendall tau B (τ) tests on the right and left sides. In the chi-square (χ²) test, the Pearson correlation value corresponding to 1 for LF was 0.292 for the right side and 0.370 for the left side in the calculation of ST; the correlation coefficient in the Kendall tau b test was 1 for LF and 0.543 for ST on the right and 0.587 on the left. In the Spearman test, the correlation coefficient was 1 for LF, 0.528 for ST for the right side, and 0.577 for the left side. The approximate b was 4.292 for Pearson chi-square (χ²), while it was 8.753 for the Spearman tests. According to these parameters, there was a highly significant relationship between both classifications. In addition, there was no statistically significant difference relative to gender or side.
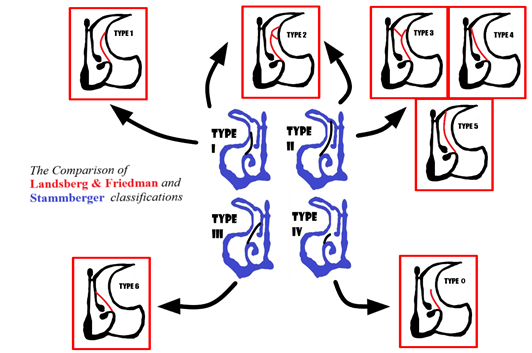
SH and LF classifications are used in assessing the SAUP of NUPs. Stammberger and Hawke first classified SAUP in 1991 [17]. In the following years, Landsberg and Friedman (1996) developed a different classification system and classified SAUPs into six groups [6]. However, since ST Type IV does not have an equivalent in LF, it was modified by adding Type 0 to the classification [16]. We observed a statistically high degree of correlation between the two groups (p < 0.01). This relationship is due to the fact that the SH groups are compatible with only some groups in LF. One-to-one compatibility was determined, respectively, between SH IV/III and LF 0/6. For other groups, such harmony cannot be mentioned, but SH I and LF 1/2, and SH II and LF 2/3/4/5 are matched. However, without seeing the CT images of the patients who were evaluated in terms of NUP, it is not possible to find the equivalent of the groups. Therefore, a comparative evaluation is also not possible between studies. Given that different classifications are used in the studies, a meta-analysis study on SAUP would be incomplete (Table 4) (Figure 3).
Table 4.
The used SAUP classification methods used in recent studies.
| Study | Classification Method |
|---|---|
| Ercan I et al. [10] | Landsberg and Friedman |
| Güngör G et al. [6] | Landsberg and Friedman |
| Srivastava M et al. [7] | Stammberger and Hawke |
| Arun G et al. [17] | Stammberger and Hawke |
| Doğan E et al. [9] | Stammberger and Hawke |
| Kansu L. [5] | Landsberg and Friedman |
| Barroso MS et al. [8] | Stammberger and Hawke |
Figure 3.
The comparison of Landsberg and Friedman and Stammberger and Hawke classifications (LF in red and SH in blue).
Figure 3.
The comparison of Landsberg and Friedman and Stammberger and Hawke classifications (LF in red and SH in blue).
Discussion
NUP is an important bone structure associated with the lateral nasal wall. It is the first anatomical structure encountered in the anterior section of the nasal cavity. It borders Hiatus semilunaris (HS) from the anterior together with the adjacent anterior ethmoid cells. The maxillary sinuses open to the posterior side of the infundibulum via the ostium [1,18,19].
There are many variations in the NUP. Less importance is attributed to pneumatisation and hypoplasia among these variations. However, pneumatisation is a relatively common one (2–14%), and when extensive, it can obstruct the anterior entrance of the nasal passage. Deviations of the NUP and SAUP are one of the factors that primarily affect the HS and PNS ostium outlets. Physiopathologically, they directly affect sinus ventilation by compressing the infundibulum [1,20,21].
The relationship of the SAUP type with the HS determines the anatomical outlet point of the frontal recess. NUP may cause pathologies by closing the ostium externally. In such cases, it is important to specify the SAUP type in the radiological reporting [22]. Frontal sinuses consist of bony anterior and posterior walls. Depending on the type of SAUP, they drain into the middle meatus or ethmoid infundibulum medially and posteriorly via the frontal recess. If NUP attaches to the lamina papyracea, the frontal sinus drains to the middle meatus via HS. If NUP attaches to the skull base or the middle turbinate, the frontal sinus drains into the ethmoid infundibulum before draining into the middle meatus [23]. In other words, the SAUP type directly affects the frontal sinus drainage path.
In addition, NUP shapes and SAUP types are associated with facial pain, rhinorrhoea, and nasal obstruction. The lateral contact of the NUP with the nasal septum or walls while reaching the roof is the main cause of facial pain. It is also involved in the aetiology of sinusitis by obstructing sinus recess and ostium. This triggers rhinorrhoea and pain [24]. Apart from the NUPs, it has been associated with many pathologies in the literature. It even has a place among the anatomic variations associated with the antrochoanal polyp [25].
NUP is closely related to the maxillary sinus ostium, as it is to the frontal sinus recess. Mostly, uncinectomy is the first step in ESS [24]. Uncinectomy is necessary for the maxillary sinus outlet during FESS [1]. There are two common types of uncinectomy techniques, known as antegrade and retrograde techniques. The basic surgical principles of both techniques are based on removing the UP to avoid a blind operation on the maxillary sinus and ostium [26]. Sickle knives or freer elevators are used in the anterograde method, while small backbiting forceps are used in retrograde uncinectomy. Aside from these techniques, other methods can be used, such as using microdebriders or other types of equipment. Knowing the SAUP type is essential, especially during the use of forceps. In the case in which the NUP adheres to the base of the skull (SH II or LF 3, 4, or 5), the base of the cranial fossa may become damaged while the uncinate process is being pulled with forceps [27]. However, it would be unfair to limit the importance of the SAUP type only to uncinectomy. Knowing the SAUP type is essential not only in uncinectomy but also in techniques for preserving the NUP for determining the maxillary ostium [28].
The orbital-related SAUP variants are important in orbital decompression operations. NUP excision is also essential in this operation technique. In LF Type 1 and 2, or SH Type I variants, it should be carefully considered against the risk of complications in the orbital interventions from inferior [29,30].
In summary, concha-related variants are the cause of facial pain. The types that adhere to the skull base are important in uncinectomy operations, and the types related to the orbit are important in orbital decompression operations.
Conclusions
The SAUP types are important in clinical and surgical management. Concha-related variants are associated with chronic facial pain. It is essential to know the types related to the skull base before uncinectomy and the types adhered to the orbit before decompression operations to avoid possible complications. NUP can fuse with some anatomic structures such as the ethmoid cell and Agger nasi cell until it reaches the insertion point. This situation can cause misconceptions by making follow-up difficult. Following the thick band and paying attention to concavity and convexity helps to accurately evaluate the anatomical structure.
SH and LF are the guides used in SAUP classifications. These two methods showed a statistically high significant correlation with each other. However, the use of different classifications in research prevents meta-analysis and causes confusion. SH Type IV/LF Type 0 and SH Type III/LF Type 6 completely overlapped. SH Type I and Type II, respectively, corresponded to LF Type 2/3, and SH Type II to LF Type 2/3/4/5 groups. There was no significant difference between males and females or between right and left, according to the LF or SH types.
Author Contributions
Conceptualisation, D.E.; Methodology, D.E.; Software, D.E.; Validation, D.E.; Formal Analysis, D.E.; Investigation, D.E. and E.C.; Resources, D.E. and E.C.; Data Curation, D.E.; Writing—Original Draft Preparation, D.E.; Writing—Review and Editing, D.E.; Visualisation, D.E.; Supervision, D.E.; Project Administration, D.E. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
We would like to thank Marwa Mouline Doğan for her help in statistical analysis and editing.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Papadopoulou, A.-M.; Chrysikos, D.; Samolis, A.; Tsakotos, G.; Troupis, T. Anatomical Variations of the Nasal Cavities and Paranasal Sinuses: A Systematic Review. Cureus 2021, 13, e12727. [Google Scholar] [CrossRef] [PubMed]
- Mokhasanavisu, V.J.P.; Singh, R.; Balakrishnan, R.; Kadavigere, R. Ethnic Variation of Sinonasal Anatomy on CT Scan and Volumetric Analysis. Indian J. Otolaryngol. Head Neck Surg. 2019, 71, 2157–2164. [Google Scholar] [CrossRef] [PubMed]
- Yenigün, A.; Cihat, G.Ü.N.; Uysal, I.I.; Keleş, M.K.; Nayman, A.; Karabulut, A.K. Prevalence of pneumatized uncinate process and accompanying neighboring variations. Turk. J. Ear Nose Throat 2016, 26, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Tuli, I.P.; Sengupta, S.; Munjal, S.; Kesari, S.P.; Chakraborty, S. Anatomical Variations of Uncinate Process Observed in Chronic Sinusitis. Indian J. Otolaryngol. Head Neck Surg. 2012, 65, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Kansu, L. The relationship between superior attachment of the uncinate process of the ethmoid and varying paranasal sinus anatomy: An analysis using computerised tomography. ENT Updat. 2019, 9, 81–89. [Google Scholar] [CrossRef]
- Güngör, G.; Okur, N.; Okur, E. Uncinate Process Variations and Their Relationship with Ostiomeatal Complex: A Pictorial Essay of Multidedector Computed Tomography (MDCT) Findings. Pol. J. Radiol. 2016, 81, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, M.; Tyagi, S. Role of Anatomic variations of Uncinate Process in Frontal Sinusitis. Indian J. Otolaryngol. Head Neck Surg. 2016, 68, 441–444. [Google Scholar] [CrossRef] [PubMed]
- Barroso, M.S.; Araújo, B.C.; Jacinto, J.; Marques, C.; Gama, I.; Barros, E. Association between the insertion type of the uncinate process and the development of Frontal Sinus Mucoceles—Is there a relationship? Acta Otorrinolaringol. Esp. 2021, 72, 246–251. [Google Scholar] [CrossRef]
- Doğan, E. Yüksek Rezolüsyonlu BT ile Erişkin Yaş Grubunda Ünsinat Proçes Anatomik Varyasyonlarının ve Maksiller Sinüs Hastalıkları ile İlişkisinin Değerlendirilmesi [Turkish]. Muğla Sıtkı Koçman Üniversitesi Tıp Dergisi 2018, 5, 4–10. [Google Scholar]
- Ercan, I.; Çakir, B.Ö.; Sayin, I.; Başak, M.; Turgut, S. Relationship between the Superior Attachment Type of Uncinate Process and Presence of Agger Nasi Cell: A Computer-Assisted Anatomic Study. Otolaryngol. Neck Surg. 2006, 134, 1010–1014. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.P.; Liu, S.Y.; Zhang, W.; Wang, Y.C.; Ji, B.; Meng, L.Y.; Liu, Y.H. [The value of “posterior approach, uncinate process priority, artery first” in laparoscopic pancreatoduodenectomy]. Zhonghua Yi Xue Za Zhi 2020, 100, 3328–3331. [Google Scholar]
- Jamieson, D.; Schwenn, P.; Beaudequin, D.A.; Shan, Z.; McLoughlin, L.T.; Lagopoulos, J.; Hermens, D.F. Short strides to important findings: A short interval longitudinal study of sleep quality, psychological distress and microstructure changes to the uncinate fasciculus in early adolescents. Int. J. Dev. Neurosci. 2020, 81, 82–90. [Google Scholar] [CrossRef]
- Kocabiyik, N.; Ercikti, N.; Tunali, S. Morphometric analysis of the uncinate processes of the cervical vertebrae. Folia Morphol. 2017, 76, 440–445. [Google Scholar] [CrossRef]
- Stammberger, H.R.; Kennedy, D.W.; Anatomic Terminology Group. Paranasal sinuses:anatomic terminology and nomenclature. Ann. Otol. Rhinol. Laryngol. Suppl. 1995, 167, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, B.N.D.F.; Muniz, B.C.; Marchiori, E. Preoperative computed tomography evaluation of the paranasal sinuses: What should the physician know?—Pictorial essay. Radiol. Bras. 2019, 52, 117–122. [Google Scholar] [CrossRef]
- Alsufyani, N.; El-Hakim, H.; Major, P. Prevalence of maxillary sinus hypoplasia and association with variations in the sinonasal complex: A cone beam CT study. Clin. Oral Investig. 2021, 25, 5463–5471. [Google Scholar] [CrossRef]
- Arun, G.; Moideen, S.P.; Mohan, M.; Afroze, M.K.H.; Thampy, A.S. Anatomical variations in superior attachment of uncinate process and localization of frontal sinus outflow tract. Int. J. Otorhinolaryngol. Head Neck Surg. 2017, 3, 176–179. [Google Scholar]
- Berger, G.; Eviatar, E.; Kogan, T.; Landsberg, R. The normal uncinate process: Histology and clinical relevance. Eur. Arch. Otorhinolaryngol. 2013, 270, 959–964. [Google Scholar] [CrossRef]
- Lakha, T.A.; Sandhu, R.; Kheur, M.G.; Supriya, M.; Valentini, P.; Le, B.; Ta, L. Anatomic variations of the osteomeatal complex and its relationship to patency of the maxillary ostium: A retrospective evaluation of cone-beam computed tomography and its implications for sinus augmentation. J. Indian Prosthodont. Soc. 2020, 20, 371–377. [Google Scholar] [CrossRef]
- Alsowey, A.M.; Abdulmonaem, G.; Elsammak, A.; Fouad, Y. Diagnostic Performance of Multidetector Computed Tomography (MDCT) in Diagnosis of Sinus Variations. Pol. J. Radiol. 2017, 82, 713–725. [Google Scholar] [CrossRef]
- Azila, A.; Irfan, M.; Rohaizan, Y.; Shamim, A.K. The prevalence of anatomical variations in osteomeatal unit in patients with chronic rhinosinusitis. Med. J. Malays. 2011, 66, 191–194. [Google Scholar]
- Jiang, W.; Xie, S.; Xie, Z.; Tang, Q.; Wu, B.; Zhang, J.; Sun, H.; Fan, R.; Xiao, J.; Zhao, S.; et al. Endoscopic frontal recess anatomy directed by the drainage pathways using the connecting plates as landmarks. Eur. Arch. Otorhinolaryngol. 2021, 278, 3315–3323. [Google Scholar] [CrossRef] [PubMed]
- Lofgren, D.H.; McGuire, D.; Gotlib, A. Frontal Sinus Fractures. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Qureshi, M.F.; Usmani, A. A CT-Scan review of anatomical variants of sinonasal region and its correlation with symptoms of sinusitis (nasal obstruction, facial pain and rhinorrhea). Pak. J. Med Sci. 2021, 37, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Gursoy, M.; Erdogan, N.; Cetinoglu, Y.K.; Dag, F.; Eren, E.; Uluc, M.E. Anatomic variations associated with antrochoanal polyps. Niger. J. Clin. Pract. 2019, 22, 603–608. [Google Scholar]
- Alromaih, S.; Sumaily, I.; Alarifi, I.; Alroqi, A.; Aloulah, M.; Ajlan, A.; Yaghmoor, F.; Alsaleh, S. Seeker Uncinectomy: A Randomized Controlled Cadaveric Trial. Allergy Rhinol. 2020, 11, 2152656720971262. [Google Scholar] [CrossRef]
- Lee, J.H. Severely Osteitic Uncinate Process: Prominent Feature. Ear Nose Throat J. 2021, 100, NP386–NP387. [Google Scholar] [CrossRef]
- Leite, J.G.D.S.; Nogueira, J.F.; Pallanch, J.; Da Costa, T.C.; Feijão, M.X.; Querido, R.D.S.L.F.; Cavalcante, M.L.C.; De Sousa, R. Lobo “M” line: New anatomical landmark for the maxillary sinus natural ostium. Clin. Otolaryngol. 2020, 45, 177–181. [Google Scholar] [CrossRef]
- Tatehara, S.; Inokuchi, G.; Takeda, H.; Kuroki, S.; Fujio, H.; Azumi, A.; Nibu, K.-I. Frontal sinusitis associated with orbital decompression for Graves’ orbitopathy. Auris Nasus Larynx 2020, 47, 1079–1082. [Google Scholar] [CrossRef]
- Spini, R.; Cruz, D.; Fernández, L.; Urquiola, F. Complicación orbitaria recurrente por rinosinusitis. Reporte de un caso. Arch. Argent. de Pediatr. 2019, 117, e670–e675. [Google Scholar]
© 2022 Copyright by the authors Licensed as an open access article using a CC BY 4.0 license